



Brief Primers on the Neuroscience of Psychedelics 4: The NMDA Antagonists (Ketamine)
Is ketamine a psychedelic? A dissociative anaesthetic? A dissociative psychedelic?

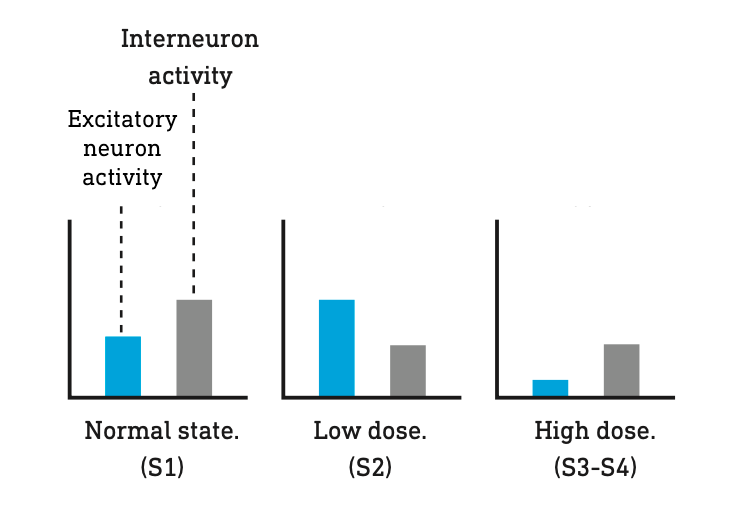
The first human was given ketamine via intravenous injection on August 3, 1964. As the dosage was gradually increased, the patient experienced the now familiar tiers of the ketamine state: from no effect at very low doses to an entirely alert but “spaced out” state and, finally, at the highest doses, an unresponsive anaesthetised state. This pattern was repeated with a number of subjects, many of whom reported feeling detached from their bodies, floating in outer space, and completely disconnected from the outside world. This sensory detachment inspired the name of what would soon become an entirely new class of psychoactive molecule with ketamine as its founding member: the dissociative anaesthetics. However, at low doses, they share many of the types of effects experienced with the classic psychedelics, including a restructuring of the world model and alterations in its relationship to the environment. At higher, more challenging doses, ketamine can also gate access to entirely new reality channels populated by intelligent entities. In line with its subjective effects, ketamine has been shown to increase neural activity at low concentrations, but shift to an overall suppressive effect on the brain as the concentration is increased.
Ketamine works by binding to glutamate-gated ion channels known as NMDA receptors in the cortex. Normally, when glutamate binds to this receptor, the channel opens and allows sodium ions to flow into the neuron, making it more likely that the neuron will fire. However, crucially, the ion channel is normally blocked by a magnesium ion and will only open fully if glutamate is bound AND the magnesium ion has dissociated. Magnesium is more likely to dissociate from the NMDA receptor when the neuron is in a depolarised (“activated”) state.

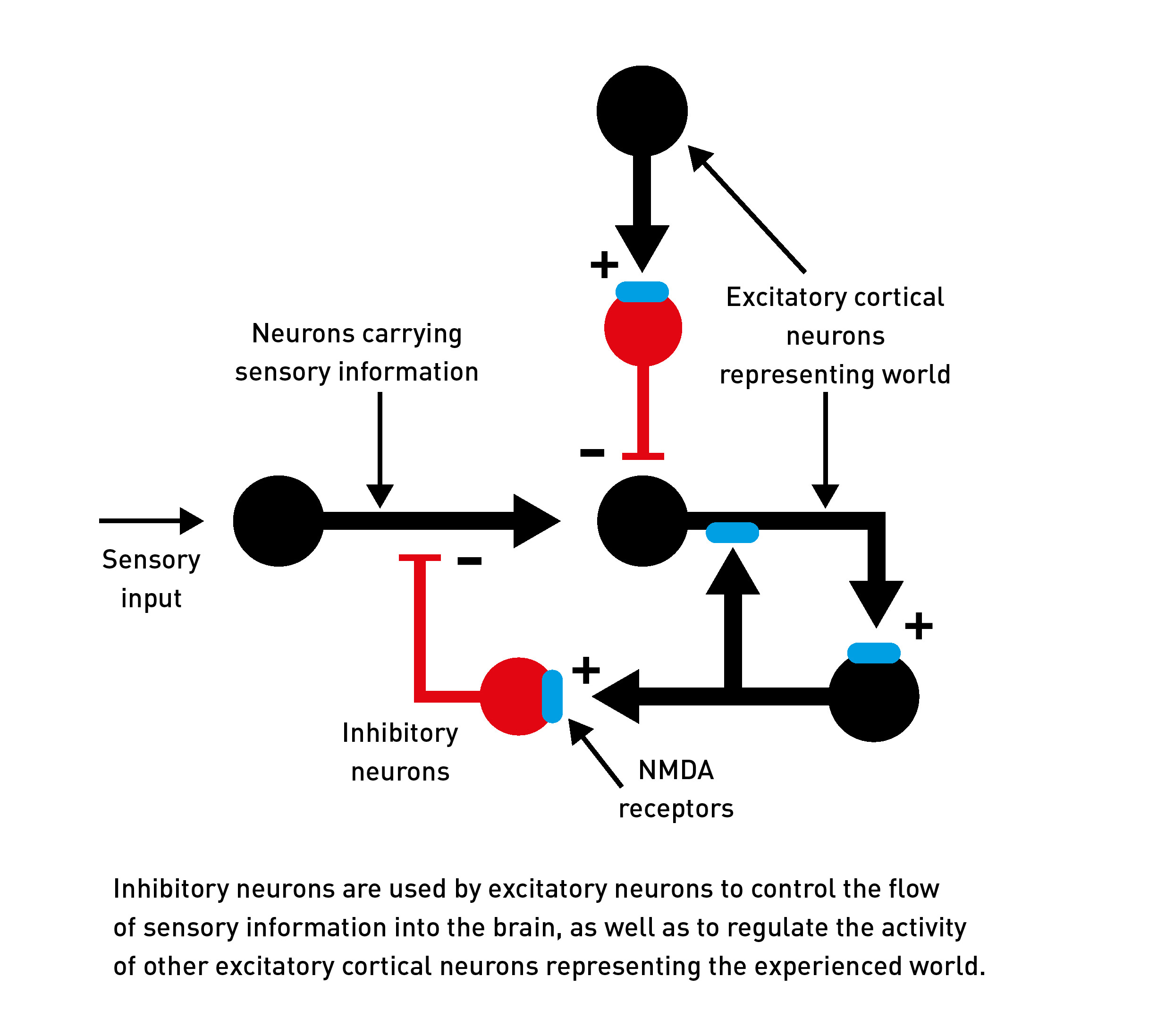
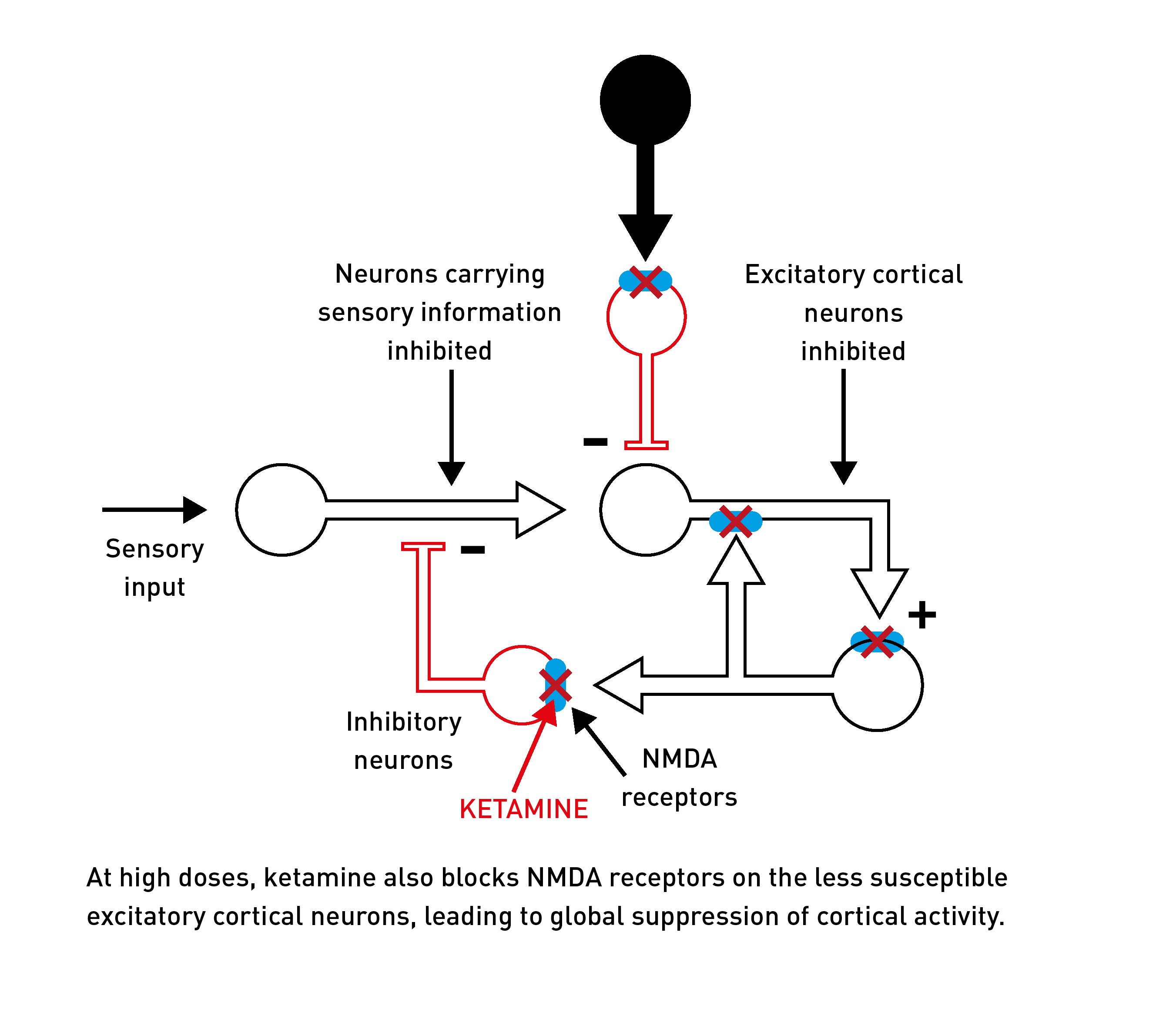
NMDA receptors are found in the membranes of neurons all across the brain, but they have important roles in regulating the activity of, and controlling the flow of information between, neurons that generate the patterns of neural activity that represent your experienced world. In particular, NMDA receptors are used by neurons that control the flow of sensory information into the brain. They are also found on inhibitory interneurons that help to control (by inhibiting) the activity of excitatory neurons across the cortex, as well as on the excitatory neurons themselves.
Ketamine sits in the ion channel part of the NMDA receptor and blocks the flow of sodium ions, even when glutamate is bound. In other words, it acts as an NMDA receptor antagonist. This exhibits what’s known as use dependence, which means the ketamine molecule can only bind and block the NMDA ion channel when the magnesium ion has been displaced. This means ketamine has a stronger effect on neurons that are already highly active, since their NMDA receptors will spend more time without the magnesium block when ketamine can bind.

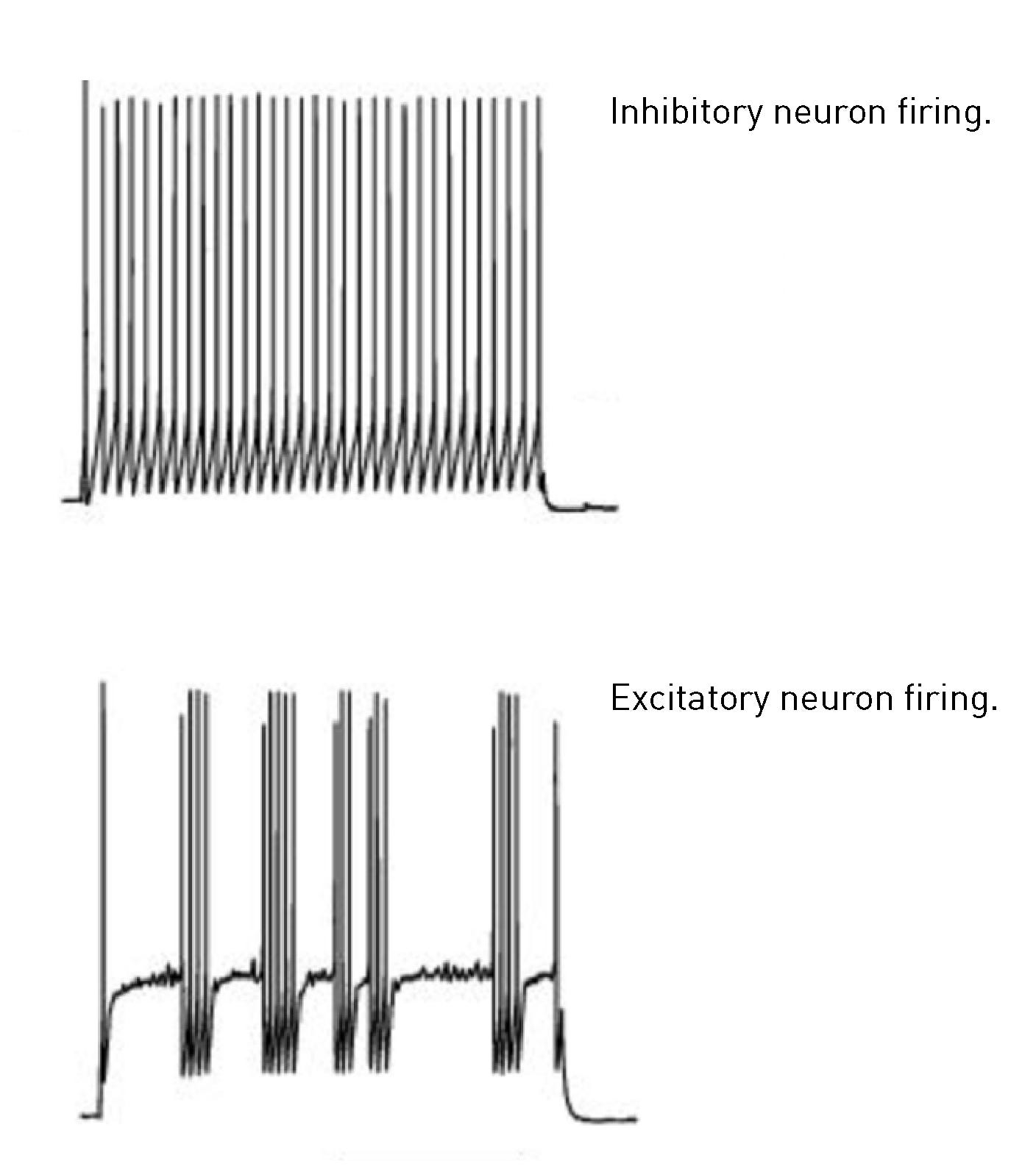
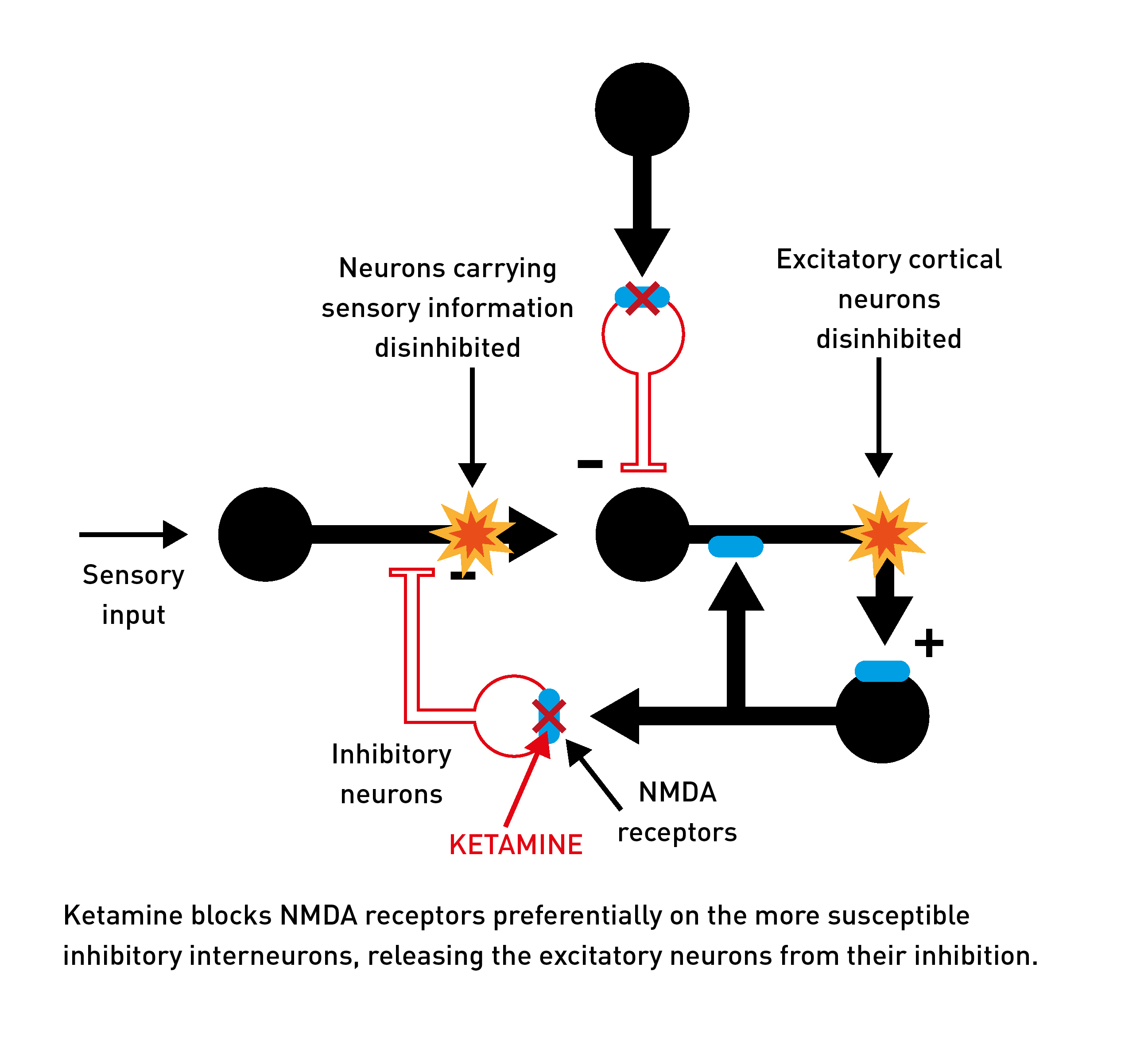
The inhibitory interneurons (that control cortical activity) tend to fire at a constant high rate, whereas the excitatory neurons are more likely to display intermittent bursts of firing. As such, the NMDA receptors embedded in inhibitory interneurons spend more time without their magnesium ion and are thus more susceptible to the effects of ketamine.
At low doses, this effect on the more susceptible inhibitory interneurons dominates, releasing the excitatory neurons from suppression (disinhibiton), resulting in an overall increase in activity across the cortex. The neurons that use NMDA receptors to control the flow of sensory information into the brain are also suppressed. So, overall, the cortex becomes more excitable and more susceptible to sensory inputs. This is similar to the effect of low dose classic psychedelics, albeit by a different mechanism, and is experienced as the low-dose psychedelic ketamine effect.
But, as the dosage is increased, ketamine begins to inhibit the less susceptible excitatory cortical neurons directly, and this suppressive effect on the cortex eventually begins to overwhelm the disinhibition caused by suppression of the inhibitory interneurons. This is experienced as the “anaesthetic” ketamine effect.
However, this type of anaesthesia is unlike that of other general anaesthetics that cause a more straightforward type of global suppression of cortical activity. Because ketamine is generating both a suppressive and excitatory effect (like a “push-pull” effect) on the cortex, a highly unusual pattern of neural activity emerges: the cortex alternates every few seconds between an active state similar to normal waking consciousness and a suppressed anaesthetised state.
The user’s (or patient’s) consciousness rapidly switches between full awareness and an unconscious state disconnected from the environment — a fragmented dream-like state of consciousness unlike that elicited by any other class of psychedelic molecule. The dosing margin of error with ketamine is quite small, and it’s plausible that the “K-hole”, in which the user temporarily experiences a highly dissociated effect, results from an accidental (or intentional) slip into this high-dose domain.

The deep anaesthetised state is often accompanied by amnesia, so it’s difficult to be definitive about when the more intense visionary states are most likely to be experienced — during the deep K-hole state or once brain levels begin to decline again. However, ketamine undoubtedly has the capacity to immerse the user in entirely new worlds which are often inhabited.
Physician and dolphin-whisperer John Lilly used ketamine extensively whilst floating in an isolation tank — he believed that the combination of the unique ketamine-induced state of consciousness lowered the threshold for receiving information from extraterrestrial intelligences. Although the interpretation of these encounters will vary, it isn’t unusual for high-dose ketamine users to be carried on journeys across fantastical landscapes to meet with a range of intelligent beings.
For a much more detailed discussion and explanation of the neurological mechanisms behind the dissociative psychedelics, please refer to my latest book, Reality Switch Technologies: Psychedelics as Tools for the Discovery and Exploration of New Worlds, which covers all the major classes of psychedelics in unprecedented depth and detail. See my website for more details:
https://www.buildingalienworlds.com/books.html
You wrote, "At higher, more challenging doses, ketamine can also gate access to entirely new reality channels populated by intelligent entities." Have you looked at the 2022 Nobel Prize in Physics which was given for showing instances of "spooky" as Einstein called them, or paranormal events at a subatomic level? The Nobel Prize winners go on to make a distinction between places which are local and places which are nonlocal. Do these intelligent entities reside in a place which is nonlocal? Or, are these intelligent entities simply fabrications of one's own imagination? What scientific criteria would you suggest to investigate and find answers to these questions?
No common examples of substances which exhibit 5HT2a agonism and NMDA antagonism… And where does the SIGMA receptors come into play?